If you think this isn’t a thing, there was a 2000 study on using a self-spreading vaccine on wild rabbit populations that was somewhat successful. They’ve been monkeying around with things for a while and putting it out into the wild. There are also two new diseases that are spread by ticks that popped up in more recent history after they started looking into insects as means of spreading biological weapons, specifically Lyme Disease and Alpha-Gal syndrome which results in a meat allergy, for which they’ve developed GMO pigs already approved by the FDA (coincidence I think not). Consequently, this is a very good write up and the free portion with the rest being for paid subscribers on A Midwestern Doctor’s Substack. And I’ll quote a couple parts I found very interesting.
At the same time however, Pfizer’s protocol for testing their vaccine:
- Prohibited pregnant women or those breast feeding from receiving the vaccine (or future doses if they had already received one).
- Stated it needed to be reported if a pregnant women (e.g., a healthcare worker in the trials) was exposed to the intervention by inhalation or skin contact from someone who had been vaccinated.
- Stated it needed to be reported if someone in the previous category (not vaccinated but exposed to someone who was) then was in close proximity to their wife and their wife was pregnant.
This suggested either that Pfizer knew shedding (and secondary shedding) was a real problem, or that they were following the existing standards—the FDA stipulates that gene therapies need to be evaluated for shedding before being given to humans (and furthermore be subsequently tested for shedding in humans). For context, both the FDA and the EMA (along with Moderna and Pfizer 1,2,3) classify the mRNA vaccines as a gene therapy.
•The vaccine’s design primarily reduces reactivity to the spike protein (i.e., COVID-19 symptoms). As such, vaccinated individuals can be infected with COVID-19 but not show symptoms of infection.
Numerous data sources now corroborate that the COVID vaccines shed in a consistent and replicable manner
By A Midwestern Doctor
Jan 19, 2025
Story at a Glance:
•After the COVID-19 vaccines hit the market, stories began emerging of unvaccinated individuals becoming ill after being in proximity to recently vaccinated individuals. This confused many, as the mRNA technology in theory should not be able to “shed.”
•After seeing countless patient cases which can only be explained by COVID vaccine shedding, a year ago, I initiated multiple widely seen calls for individuals to share suspected shedding experiences.
•From those 1,500 reports, clear and replicable patterns have emerged which collectively prove “shedding” is a real and predictable phenomenon that can be explained by known mechanisms unique to the mRNA technology.
•Likewise, after being blocked from publication for over a year, recently, a scientific study corroborating the shedding phenomenon was finally published.
•This article will map out everything that is known about shedding (e.g., what are the common symptoms, how does it happen, who does it affect, does it occur through sexual contact, can it cause severe issues like cancer) along with strategies for preventing it.
When doctors in this movement speak at events about vaccines, by far the most common question they receive is, “Is vaccine shedding real?”
This is understandable as COVID-19 vaccine shedding (becoming ill from vaccinated individuals) represents the one way the unvaccinated are also at risk from the vaccines and hence still need to be directly concerned about them.
Simultaneously, it’s a challenging topic as:
•We believe it is critical to not publicly espouse divisive ideas (e.g., “PureBloods” vs. those who were vaccinated) that prevent the public from coming together and helping everyone. The vaccines were marketed on the basis of division (e.g., by encouraging immense discrimination against the unvaccinated), and many unvaccinated individuals thus understandably hold a lot of resentment for how the vaccinated treated them. We do not want to perpetuate anything similar (e.g., discrimination in the other direction).
•We don’t want to create any more unnecessary fear—which is an inevitable consequence of opening up a conversation about shedding.
•In theory, shedding with the mRNA vaccines should be “impossible,” so claiming otherwise puts one on very shaky ground.
Conversely, if shedding is real, we believe it is critical to expose as:
•Those being affected by it are in a horrible situation, particularly if everyone is gaslighting them about it and insisting it’s all in their head.
•It provides one of the strongest arguments to pull the mRNA vaccines from the market and prohibit the widespread deployment of mRNA technologies in the future.
For those reasons, Pierre Kory and I have spent the last year and a half trying to collect as much evidence as possible to map out this phenomenon with the following data sets:
•Dozens of extremely compelling patient histories1,2,3 from Kory and Marsland’s medical practice, including many responding to spike protein treatment.
•My own experience with patients and friends affected by shedding.
• I read large numbers of reports of shedding in (now deleted) online support groups.
•Roughly 1,500 reports from individuals affected by shedding we were able to collect.
•Extensive menstrual data compiled by MyCycleStory.
From that and the hundreds of hours of work that went into it (particularly reviewing and sorting the 1,500 reports), we can state the following with relative certainty:
1. Shedding is very real (e.g., each of those datasets is congruent with the others), and many of the stories of those affected by it are very sad.
2. People’s sensitivity to it dramatically varies.
3. Most of the people who are sensitive to shedding have already figured it out.
4. Mechanistically, shedding is very difficult to explain. However, now that new evidence has emerged, a much stronger case can be made for the mechanisms I initially proposed a year ago.
Note: if you have a shedding experience you would like to share (or wish to read through them), please do so here, where they are compiled.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber. To find out how others have benefitted from this newsletter, click here!
Shedding Overview:
By far, the most common symptom of shedding is unusual and disrupted menstrual bleeding (which is also the most common COVID vaccine injury). This in turn, was the first thing that alerted me to the inconceivable possibility the vaccines could shed, as I quickly received many similar reports of highly unusual menstrual bleeding, which appeared to be due to exposure to someone who was vaccinated.
After this, the most common symptoms were headaches, flu-like illnesses, nosebleeds, fatigue, rashes, tinnitus, sinus or nasal issues, and shingles. Other less frequent symptoms are also repeatedly seen (e.g., palpitations, herpes outbreaks, and hair loss).
Additionally, many noticed they could immediately tell when they were in the vicinity of a shedder, typically either due to noticing a unique odor or symptoms immediately onsetting.
Generally speaking, the character of shedding symptoms were quite similar to long COVID and vaccine injuries, but typically were more superficial in nature, suggesting the body was reacting to a harmful external pathogenic factor rather than one already deep inside the body. More severe issues (e.g., cancers or heart attacks) also occurred, but these were much rarer than what you saw in the vaccine injured population, again suggesting shedding was primarily an external reaction. Interestingly, most of the (fairly varied) shedding symptoms overlap with the conditions DMSO treats (e.g., strokes), suggesting that DMSO’s key mechanisms of action (e.g., increasing blood flow, eliminating large and small blood clots, being highly anti-inflammatory, and rescuing cells from the cell danger response) are the exact opposite of what shedding does to the body.
Note: in the following sections, each superscript citation links to individual reports I’ve received about the phenomenon. I provided these citations to show how frequent many of these effects were, so that those who’d experienced them could see many others had too, and so that anyone who wants to research this has access to the primary data. The only shedding symptom I avoided comprehensively citing was abnormal menstruation, as so many reports were received, it was not feasible to compile all of them.
Shedding Patterns
In the same manner that there is a fairly high replicability in the symptoms individuals who are affected by shedding experience, there is also a fairly high congruency in the patterns of how they are affected. Specifically:
1. Some individuals are hypersensitive to shedders and can immediately detect when they are in the presence of a shedder or are on their way to developing harmful symptoms.
2. Others are less sensitive, but quickly notice specific characteristic symptoms consistently occur following shedding exposures (e.g., always feeling ill when a vaccinated husband returns from a long trip away, when going to church each week, when singing with their choir, or when taking a crowded route to work).
In some cases, they are able to identify a “super shedder” (amongst a group) who consistently made them ill, and in many cases they can identify the exact shedding incident that made them ill. Likewise, through tracking serial spike protein antibody levels (e.g., for patients undergoing treatment for long Covid or a vaccine injury) we’ve objectively corroborated that shedding exposures repeatedly worsen these patients (providing an explanation for why their symptoms “inexplicably” ebb and flow), that this can be seen objectively in their lab work and that spike protein treatments after shedding exposures clinically improve these patients.
Note: Pierre Kory’s practice has been able to determine that those they suspect are a shedder (e.g., a husband) test positive (through an antibody test) for a high spike protein levels and that eliminating the shedder from the patient’s life or treating the (asymptomatic) shedder with a vaccine injury protocol frequently significantly improves their patient’s recovery. Likewise, readers here have reported significant improvements from avoiding shedders—which sadly in some cases has required the more sensitive individuals to isolate themselves from society.
3. In the majority of cases, the effects of shedding are temporary and go away, but in a subset of people, they can last for months if not years.
4. Recognition of the shedding phenomenon has forced many to significantly change their lives. This included regretfully terminating a long-term romantic relationship, leaving their line of work (e.g., some massage therapists can no longer handle working on vaccinated clients), or only seeing unvaccinated healthcare providers (e.g., numerous people reported getting ill from vaccinated chiropractors or massage therapists, and we now periodically will have patients state they can only see us if we are unvaccinated).
5. The “stronger” the shedding exposure, the more likely shedding is to cause issues, but conversely, for more sensitive patients, “weaker” exposures also will. More substantial exposures include being around someone who was recently vaccinated or boosted (as shedding is strongest initially), being around more shedders, being in a confined space (e.g., a car) with a shedder for a prolonged period, or having close physical contact with a shedder.
Note: given all of this, I thought flying on airlines would be a significant issue, but I have only received two reports from readers where this was the case.
6. There appear to be some unexplained symptoms otherwise healthy patients now experience that are tied to shedding. However, it’s still often very challenging to tease out when shedding is the culprit due to how many variables are involved and the ambiguity of the subject (which is part of why so much detail has gone into this post so each of you can figure out if you are being affected by shedding).
Susceptibility to Shedding
In general, there are three categories of people who are susceptible to shedding (and in many cases these categories overlap).
The first are the sensitive patients (e.g., those who frequently react to chemicals or get injured by pharmaceuticals). For example, near the start of the vaccine rollout (before I was aware that shedding was an issue), I saw this video and genuinely wondered if it was real as many of its claims were quite extraordinary but at the same time, were somewhat in line with what a highly sensitive patient (of whom I know many) would describe.
However, I’ve since received numerous accounts from sensitive patients identically matching hers along with similar but less extreme cases,123456789101112131415161718192021222324252627282930313233 such as a sensitive osteopath who can no longer see unvaccinated patients, or a susceptible nurse who shared: “I am so distraught. I went to school and trained for this work. I loved caring for my senior community, and now they’re all Covid vaccinated.”
Additionally, many of these individuals pointed out that they had the MTHFR genetic polymorphism, and attributed their sensitivity to it.12345678 While this is likely true (as MTHFR has long been observed to increase one’s likelihood of a vaccine injury), I am unsure how useful this data point is as there are many different MTHFR mutations that create varying susceptibilities (e.g., 60-70% of the population has an MTHFR mutation but most are not of the type that creates hypersensitivities).
Note: as I discuss here, sensitive patients are largely neglected and unrecognized by the medical system but frequently encountered in clinical practice. Typically in addition to being sensitive to environmental toxins or medical interventions, they are also very empathetic and aware of subtle human (or animal) qualities others miss. Generally, they tend to have an ectomorphic or Satvic constitution and are hypermobile (which as discussed here, plays a key role in why they tend to frequently experience vaccine injuries). Since publishing those articles, many readers here have shared they belong to that archetype and are more frequently injured (e.g., by shedding).
Due to these susceptibilities, those patients frequently have chronic illnesses such as mast cell degranulation disorder, multiple chemical sensitivities, EMF sensitivities, Lyme disease, mold toxicity, and fibromyalgia. These patients were more likely to avoid the COVID-19 vaccine (due to their previous bad experiences with pharmaceuticals) and more likely to be chronically debilitated by the COVID vaccine (or a COVID-19 infection). Tragically, we’ve also seen many people develop these sensitivities after a COVID-19 vaccine injury, and a few people have shared spike shedding caused them to develop environmental sensitivities (e.g., this reader lost the ability to eat meat—something I had previously only seen after tick borne diseases). Additionally, I received a report from someone who noticed environmental EMFs worsened their sensitivities to shedding.
The sensitive patients tend to be the most susceptible to shedding. I’ve seen numerous reports of individuals (e.g., consider this report from one of Pierre Kory’s patients) who can immediately tell if they are around individuals who have been vaccinated (e.g., because they immediately feel a “toxic” presence or feel a shedder injure them). Likewise, these patients tend to become ill from “weaker” shedding exposures.
Note: I consider myself to be a sensitive individual, but I have not had any issues being in close proximity to people (e.g., patients) who were recently vaccinated. Conversely, many of my sensitive female friends (who are less sensitive than me) have experienced notable effects from shedding (e.g., menstrual abnormalities), which suggests to me there is more to this picture than just having a “sensitive” constitution.
The second group is patients sensitized to the spike protein due to a previous vaccine injury or long COVID. These patients frequently find their symptoms worsen when they are around vaccinated individuals, and many have reported that their sensitivity to shedding increases with time.
Note: I believe the Cell Danger Response (discussed here) provides one of the best models to explain what happens to the patients in the first two categories (e.g., a persistent CDR accounts for many environmental sensitivities while conversely, treating the CDR is often very beneficial to these patients). Likewise, I also find a pre-existing impairment in zeta potential (discussed here) frequently predisposes these patients to these issues and that restoring the physiologic zeta potential often greatly benefits them. Finally, since the spike protein is an allergen that is highly effective at creating autoimmunity in the body, that also can explain why successive exposures to it increase one’s sensitivity to it (and likewise some of the most promising COVID-19 treatments simply use allergy medications).
The third group are the people who cannot effectively produce antibodies to the spike protein. I was initially clued into this from a study of vaccinated patients who developed myocarditis, which discovered that (unlike controls) their ability to develop a neutralizing antibody for the spike protein was impaired, leading to free spike protein circulating in their blood (whereas normally it would be bound to an antibody). Because of this, the spike protein being produced in their body is thus able to create havoc throughout it, and those patients become symptomatic after being exposed to a much lower concentration of the spike protein. It is important to note that while reactive to shedding, these patients are nowhere near as sensitive to shedding as the previously described “sensitive patients.”
Note: at the time of the disastrous smallpox campaign, many clinicians believed that those with a weakened immune system could not mount a response to the vaccine and in turn, were both more likely to be injured by it and to catch smallpox (both before and after vaccination). This led them to argue the vaccine’s “efficacy” was an artifact of the skin reaction it caused being a proxy for a functioning immune system, and I suspect the 2023 myocarditis study suggests something similar is occurring for the spike protein vaccines.
Additionally, while very rare, I have received a few compelling cases that suggest pets (e.g., cats, dogs, and parrots) can also be susceptible to shedding events..12345678910111213 If shedding did indeed happen there, it suggests that like human beings, certain animals are much more sensitive to shedding than others, and that the shedding agent has a mechanism of harm which is not dependent upon a human receptor (e.g., it adversely affects the physiologic zeta potential).
Note: since most of the symptoms of shedding are tricky to observe externally (e.g., fatigue or dizziness), it’s also possible that the “lower” incidence of shedding in pets is party due to only rarer events (e.g., cancer, heart attacks or hair loss) being observable by the owners, and that a much larger number of less severe shedding injuries have gone unrecognized.
Characteristics of Shedders
The most common observation with shedders is that they are dramatically more likely to shed soon after vaccination (depending on who you ask, this window ranges from three days to four weeks). However, more sensitive patients find they are affected by a shedder indefinitely and strongly disagree with a 2-4 week cutoff.
I believe this essentially matches what has been found in numerous studies—that following vaccination, spike protein production in the blood spikes and then declines but never reaches zero and appears to continue for months afterward.
Note: presently we do not know how long spike protein persists in the body as the vaccine mRNA was designed to resist degradation, and in each window that’s been looked at (e.g., 28 days, 30 days, 56 days, 187 days) the spike protein is still present in a portion of vaccine recipients. In fact, (still unpublished) research found it at 709 days post vaccination.
Additionally, quite a few people have noticed that shedding events (in the same location) are the most frequent and severe immediately following a new booster rollout, after which they gradually diminish until the next booster campaign.
It has also been observed that young and healthy people tend to shed more frequently (presumably since their body has a greater capacity to manufacture the spike protein), children shed the most, and the elderly shed the least frequently. Additionally, quite a few people have observed that shedding greatly varies by the individual (e.g., “I react to specific people I see at church”).
Repeatedly boosting appears to worsen shedding for three reasons:
•It causes patients to temporarily resume having high spike protein levels in their body.
•Successive boosting appears to increase the degree of shedding, which occurs when compared to what was caused by the previous injections.
•Quite a few holistic healers have shared that they believe the most recent boosters are more potent and hence cause more significant shedding than the earlier ones (which might be explained by the boosters now containing multiple strains of mRNA to cover the new variants).
In almost all cases, the shedding appeared from mRNA gene therapies. However, a few readers shared common shedding symptoms were triggered by J&J1234 or AstraZeneca.12
The Shedding Odor
One of the odd things quite a few people have reported is a distinct smell which emerged around them after the vaccines entered the market. For example, consider this comment from a reader:
In terms of crowds… I too have experienced this many times. I feel unwell with flu like symptoms and can smell a unique ordour around people. After feeling this way and smelling the same ordour several times in company with family and friends, I confirmed the correlation with the covid vaccination. As it transpired each has been vaccinated within the previous week. I am very sensitive to meds and in general and I swear I can smell something so now I ask and yep the link is there!
I have received a variety of similar descriptions of the smell itself.12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455
The labels I’ve seen used to describe the smell are as follows (with those in bold being the ones more commonly reported): “mild sickly sweet,” “rotting [or dying] flesh,” “magnetic onion,” “unpleasant,” “distinctive,” “the smell of death,” “medicines plus latrines,” “musty,” “musty plus rancid” “dead animal,” “a decomposing body,” “road kill,” “putrid meat,” “like ammonia but not as strong,” “sweet,” “sour stomach” “elderly person as their flesh breaks down with age,” “a chemical flu smell” “of seaweed,” “putrid,” “sweet meat” “strange and metallic” “sharp, pungent and toxic” “horrible” “unique odor” “chemical,” “sharp chemical,” “vinegar,” “sour,” “subtle like a pheromone,” “chemical floral,” “foul and sweet,” “acid smell,” “similar to smell chemotherapy patients have,” “horrendous breath,” “overpowering.”
From investigating this odor (which I personally cannot smell) I’ve learned:
•The three things that most closely match the odors described here are trans-2-Nonenal, malondialdehyde, and rotting organic matter—all of which can naturally occur in the body, suggesting the shedding odor to some extent represent spike protein tissue injury, and to some extent are congruent with the observation the vaccine often causes accelerated aging.
•The other “chemical” smell-sensitive individuals have started observing throughout the environment, which may be from molds in the environment metabolizing the shedded spike protein or the disinfectants sprayed everywhere throughout COVID-19.
•A higher spike protein load appears to be “easier” to smell (e.g., in someone recently vaccinated—as spike protein levels spike in the blood after vaccination, if the shedder has had a higher total number of COVID vaccines, when in close proximity to a shedder particularly if some type of intimate contact occurred, or when around someone who for some reason sheds to a greater degree). Similarly, more sensitive people (who are typically more likely to be injured by the vaccines) are more likely to detect this smell (e.g., they can still smell it once the shedders are no longer physically present), and in many cases can consistently tell if someone was vaccinated.
•Given that dogs can detect COVID-19 infections with a high degree of accuracy (e.g., one study found they could spot it in sweat samples from infected individuals two days earlier than PCR tests and with a 97% accuracy), dogs could most likely also easily be trained to detect shedders. However, to my knowledge, this has not yet been done.
•Given the previous, I am curious if individuals who can smell shedders also noticed that smell from COVID-19 (especially before the vaccine hit the market). As I did not specifically solicit it, only one reader thus far has reported it (an acid-burning smell both times they got COVID), so if you have as well, please let us know.
Note: oddly as I was working on this article, a friend at dinner shared that their body felt as though something metallic, grainy, and synthetic was in it when they had COVID.
•Individuals who can smell this will likely lose their attraction to shedders (as appealing smells are often the most important thing for sexual compatibility).
•A very perceptive colleague who can smell this reports that it appears to be being emitted through the pores, which is consistent with the evidence suggesting the shedding occurs through the sweat since it contaminates sheets.
I’ve also found cases where:
•Secondary shedding could be smelled.
•A sexual partner lost their distinctive odor.
•A few individuals with a vaccine injury could smell the shedding odor on themselves (especially in armpit sweat), and some of them noticed it worsened as their symptoms flared.1234
In certain cases, individuals perceived the shedding odor through a different sense. These included:
•Since smell is intimately linked to taste, I expected to receive reports resembling the smells. However, almost all of them were simply a “metallic taste,” with the only additional qualifiers being one who found it “unpleasant” and one who had a “dry acid feeling on my tongue.”1234567. While a metallic taste can represent many things, its frequent association with mold toxicity caught my attention.
Note: in the FOIA’d V-safe free-text data, many disclosed that they noticed a metallic taste following COVID vaccination (e.g., in the first batch of reports, 2346 respondents reported it, whereas for comparison, 15,786 vaccine recipients reported dizziness or vertigo).
•One reader felt as though their nose was inhaling glass shards, suggesting that shedding nosebleeds may be due to whatever is shed damaging superficial blood vessels. Likewise, another noticed inhaling shedder’s sweat caused their lungs to be “on fire like pins and needles,” another reported feeling as though they had inhaled some type of particulate from the air, could not stop coughing, and started feeling sick almost immediately, and a fourth feels shedding in his eyes (and also sneezes).
•One reader reported a hard and painful substance formed inside their nostril from fluid dripping through the pores in the nose and eventually coalescing into a difficult to remove stalactite (which may have been due to a zeta potential collapse of those nasal secretions).
•A few sensitive individuals a distinct energetic “aura” shedders had.12345678Most commonly, it was described as “metallic,” but also repeatedly as “heavy,” “dark,” “thick,” “black,” or “grey.” Additionally, individuals described becoming disconnected from the shedder, becoming unable to feel them, and having a dullness of mind—much of which is congruent with “brain fog.”
•One reported overwhelming dread around the shedders, while numerous readers have reported anxiety,12345mood changes, and depression1234 from shedding (some of which I suspect is due to either internal fluid stagnation or heart damage).
Note: there was a case where an “incredibly spiritual” massage therapist said she could not pray for 2 years after working on a series of vaccinated clients.
Routes of Exposure
There appear to be three possible routes of exposure.
1. General proximity to the vaccinated person—this is most likely respiratory in nature and the most common form of shedding exposure reported by patients (e.g., this reader believes the shedding traveled through an air vent). However, I have seen a few reports which suggest places which are separated by barriers (e.g., being inside a car near a crowded intersection) can also produce that exposure. Additionally, many have said shedding can be greatly mitigated outdoors or in rural areas.
2. Through skin to skin contact (e.g., hugs 12345678910111213141516171819or someone grabbing their arm). Often patients report difficulty around vaccinated individuals, but notice things become much worse once physical contact occurs, especially prolonged physical contact. Additionally, I have seen multiple cases where shedding reactions were more significant in the parts of the body touched by the shedder (e.g., a bruise, a rash, or a cancer) than those away from it.
Note: many suspect this is due to something being “shed” in the sweat.
3. Additionally, I have seen a few reports where the shedding effect appeared transferable (e.g., someone touched an object a vaccinated person touched like a phone and then became ill). Sadly, I have also come across multiple reports of cleaners noticing a distinct difference in areas shedders had been in12345 (e.g., they get sick in those environments—possibly from touching surfaces that were shed on, they can smell the shedding smell, or they notice sheets the vaccinated individuals slept in have a slightly yellowish tint). Additionally, one reader shared that they can no longer tolerate going to public restrooms due to shedding, while another shared they got ill from sleeping in sheets a vaccinated individual slept in.
Note: Individuals I trust have stated spike protein is excreted in the sweat. However when I investigated this, I could only locate research which suggested it was (as secretions occurred in analogous situations), but I could never find a study which directly measured the presence of vaccine spike protein in sweat.
There is also some evidence shedding occurs in other human secretions. This has been most clearly shown with vaccine mRNA being packaged into exosomes repeatedly being found in breast milk after vaccination (e.g., see this, this, and this study), but there is some evidence suggesting it applies to other secretions (e.g., sweat or saliva) as well. Additionally, there have been concerning infant reactions to breast milk from vaccinated mothers within VAERS and far more in Pfizer’s adverse event collection system (further discussed within this excellent article), which suggest some form of toxicity is being transmitted via the breast milk. Additionally, a study published a year ago in JAMA found that 3.5% of women reported a decrease in breast milk supply and 1-2% reported “issues with their breastmilk-fed infant after vaccination.” Oddly, however, while breast milk shedding is the most “proven” type of shedding, I have not received any reports of this (which may in part be due to the fact the readers here were unlikely to be vaccinated individuals who also breastfed their children).
Secondary Shedding
There are two forms of shedding: primary (where someone gets ill from being around a vaccinated person—e.g., vaccinated parents making their unvaccinated children ill) and secondary (where someone gets ill from being around an unvaccinated person who was recently around vaccinated people). Primary shedding is much more common, but secondary is also sometimes reported (particularly for sensitive patients).
Secondary shedding can happen with both individuals who became ill from a shedder (more common) or from someone who was not affected by a shedder (e.g., unvaccinated asymptomatic children affecting their parents after coming back home from school). Secondary shedding is one of the most confusing aspects of this phenomenon as I don’t feel many of the mechanisms I’ve proposed to explain why shedding is happening can account for secondary shedding.
Additionally, I have seen a few reports where the shedding effect appeared to transfer through inanimate objects (e.g., someone touched an object a vaccinated person touched, like a phone and then became ill). Sadly, I have also come across multiple reports of cleaners noticing a distinct difference in areas shedders had been in1234567 (e.g., they get ill in those environments—possibly from touching surfaces that were shed on and some can smell the shedding smell or notice sheets the vaccinated individuals slept in have a slightly yellowish tint).
Similarly, one sensitive reader noticed they could smell the shedding odor on clothes that came into contact with a shedder until they were washed. Likewise, readers have reported needing to clean the dust out of their house, spray down their home with water and vinegar or sanitize clothes to stop being affected by secondary shedding. Finally, one reader shared that they can no longer tolerate going to public restrooms due to shedding, while another shared they got ill from sleeping in sheets a vaccinated individual slept in. Lastly, while I’ve received many reports of individuals becoming ill after receiving a massage, acupuncture, or chiropractic adjustment from a shedding therapist, I have only found one (somewhat severe) case where this was instead due to the previous client being a shedder (suggesting it is not necessary to exclude vaccinated patients from your practice to protect other patients who are sensitive to shedding).
Finally, shedding does not appear to be an issue a major issue in pools (I have only received one report of someone getting ill from swimming with vaccinated people) but have received two reports of shedding being an issue in hot tubs.12Additionally, I have received one report of a reader being affected by being in a sauna that a likely vaccinated person had previously been in and another one from swimming (which is hard to draw any conclusions from).
Timing of Exposure
There seem to be three common variants of exposures:
•Immediate—Individuals who experience this tend to either feel as though some type of poison had been immediately injected into them, or that there is an oppressive presence in the area they are entering which makes them feel unwell.
Note: I presently suspect this form occurs in the most sensitive patients as the symptoms experienced in concurrence with that “oppressive presence” are often quite similar to what mold-sensitive patients experience in moldy rooms and EMF-sensitive patients experience in high EMF areas.
•A 6-24 hour delay—This seems to be the most common variant. In certain cases, patients have reported this occurring like clockwork (e.g., every Monday they or a relative gets ill after they had gone to church on Sunday).
•A long-term delay—This is often seen in the individuals who have the most severe complications from vaccine shedding.
In each of these cases, those affected will typically recover after a few days, but there were also many who reported a permanent (partial or debilitating) illness after the shedding exposure.
Note: in many cases the timing between shedding exposures and shedding symptoms makes it difficult for any alternative explanation to explain the chronology. This reader for example, had menstrual hemorrhages, and her period stop for 5-6 months all 4 times her husband was vaccinated (even when she was unaware he had been vaccinated)—symptoms she had never otherwise experienced in her life. Likewise, to quote another person “I was dubious about shedding till it happened to me.”
Bleeding and Menstruation
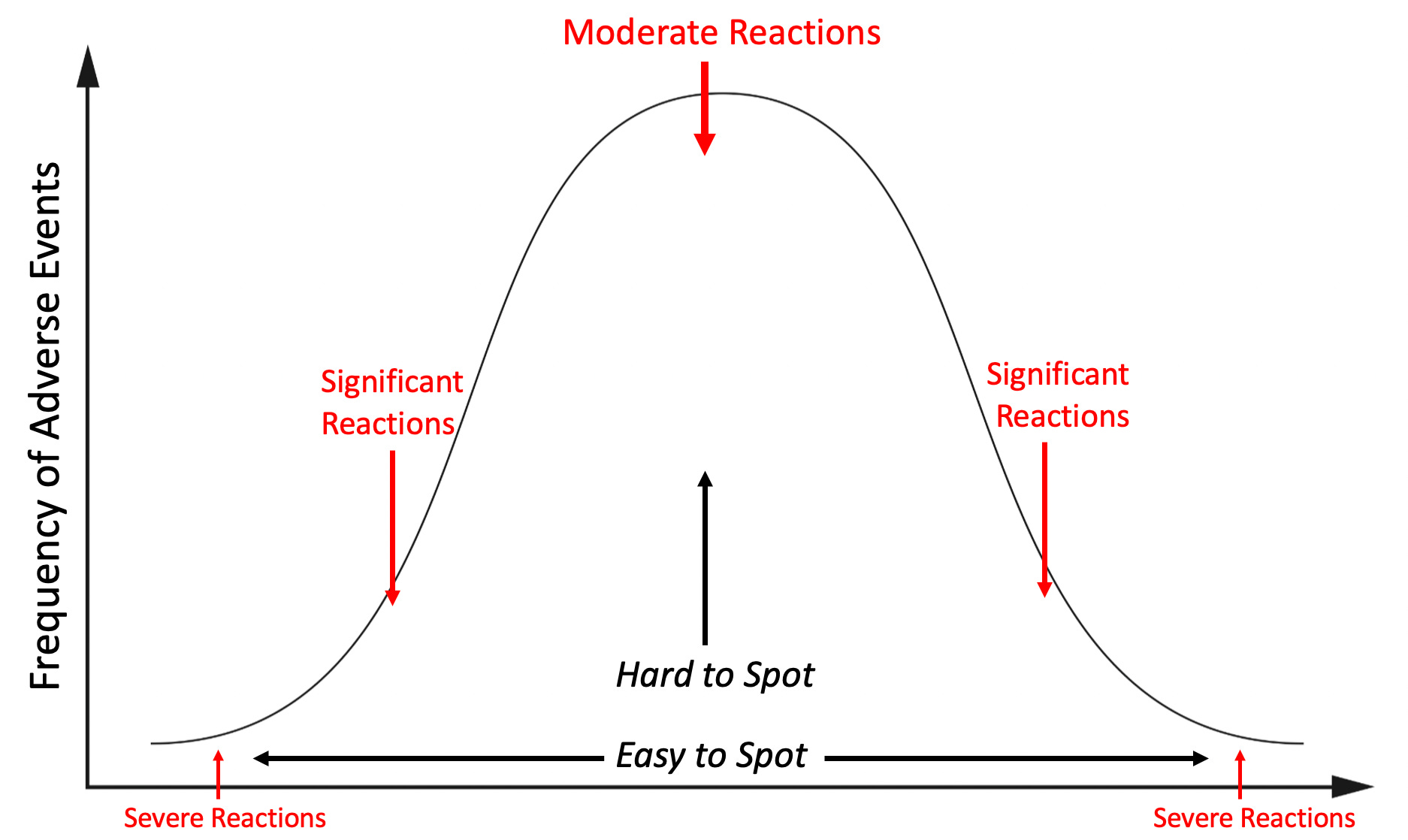
One of my general beliefs is that extreme reactions (e.g., sudden cardiac death) are much rarer than minor reactions (e.g., temporary chest pain). As such, if you observe a large number of minor reactions from a pharmaceutical, it indicates a certain number of extreme reactions are occurring, and conversely, if you see a few extreme reactions, it indicates a large number of minor reactions are occurring.
This for example, is why after I started receiving startling phone calls from people around the country after the COVID-19 vaccine hit the market of sudden death following vaccination I realized a significant number of my patients going forward would have long-term complications from the vaccine. Conversely, while none of the mRNA vaccine clinical trials reported menstrual abnormalities (nor did the CDC monitor for them), I saw more people than I can count who developed menstrual abnormalities after vaccination—something the media relentlessly denied and social media companies aggressively censored (e.g., see this article about Instagram deleting a large Instagram thread on shedding affecting female menstruation). Suspecting this side effect was being deliberately covered up, I was not surprised to learn:
•That within 4 months of the vaccines coming out, so many reports of vaccine induced menstrual abnormalities had emerged that researchers began collecting them,
•A 2022 study of 14,153 women found 78% experienced menstrual changes from vaccination.
•A 2022 study (of over 165,000 women) found that 42% of them with normal menstrual cycles had menstrual changes from vaccination, that 71% of those on long-acting reversible contraceptives did, and 66% of menopausal women did.
•A 2022 prospective study of 3858 women found vaccination made them 67% more likely to have prolonged menstruation (and 41% more likely for it to continue past 9 months), and the increase went up to 182% for those with already abnormal menstruation.
•A 2023 study found vaccination extended menstrual bleeding by 2.5 days.
•A 2023 study of 21925 non-menstruating women found vaccination increased their likelihood of bleeding by 2-5 times and that Moderna was 32% more likely than Pfizer to do this (as Moderna used a higher mRNA dose and was shown to have a higher risk of a variety of side effects including death).
•Information obtained from the free-text field in V-Safe (the CDC’s system to monitor adverse effects from the COVID vaccines) found that 62,679 women had reported menstrual irregularities from vaccination. Since this was in the free-text field (rather than something women could select) the actual number was likely far higher.
In short, the fact that roughly half of the women who received the vaccine experienced (often severe) menstrual abnormalities, but the medical field has refused to acknowledge this issue helps to explain why the trust medicine has worked for decades to build is rapidly declining in a manner I’ve never seen anything comparable to during my lifetime (going from 71.5% at the start of 2020 to 40,1% in 2024).
Note: since COVID-19 is frequently blamed for vaccine injuries, it’s worth noting that this study found COVID-19 infections only had a negligible impact on menstruation and this study found that it had no impact.
In the case of abnormal menstruation after shedding (along with many other shedding symptoms), I saw a similar pattern from the readers here (and in numerous large online support groups I’d belonged to—which were subsequently deleted). Many unvaccinated women reported unpleasant menstrual changes (to the point there are too many for me to list here) after shedding exposures, but smaller numbers reported increasingly unusual and severe symptoms.
For example, at least 60 postmenopausal readers (who should not menstruate) reported abnormal bleeding and menstrual cramps starting after a shedding event—something I also observed in quite a few of my own patients.1234567891011121314151617181920212223242526272829303132* 33343536373839404142434445464748495051525354555657585960
This for example, was reported by an 80 year old reader:
Subsequently, I had an episode of uterine bleeding for which a uterine biopsy was deemed necessary. The cervix was plugged and there was fluid in the uterus. The doctor had no experience with this kind of problem.
Additionally, I’ve received cases of shedding triggering menstrual bleeding in women as young as 8-9 years old and as old as 92 to 95 years old, bleeding in someone who’d had a uterine ablation, menstruation coming back after an IUD had eliminated it,12severe period pains triggering in women who’d had hysterectomies1,2, and severe cramps without bleeding in post menopausal women.123
Note: the fastest onset I’ve come across of this was one reader who was not currently menstruating, but after roughly 30 minutes of being around vaccinated individuals had visibly stained her white dress red.
In some cases this bleeding is so profuse it either resulted in the individual having massive clots they’d never seen before (e.g., many are described as large and jelly-like), them developing anemia from the bleeding,123and in one case needing to go to the ER because of it. This chiropractor for example, had many debilitating shedding symptoms onset after seeing patients, which then evolved into back pain, and immense menstrual bleeding every two weeks (e.g., massive clots, blood continually going through her clothes, needing to change a Diva cup every hour, periods lasting 17 days, and before long severe fatigue setting in which may have been due to anemia), all of which improved once she isolated from the vaccinated for 5 months, and then immediately resumed once she saw patients again.
One of the most unusual events we encountered (initially in those support groups) was decidual cast shedding (the entire lining of the uterus coming off as one piece)—a condition so rare that one paper that looked into this found before the vaccines, less than 40 cases of it had been reported in medical journals across the world. Since then:
•I met someone this happened to, and Pierre Kory had a patient it happened to as well.
•Numerous readers shared it happening to them.12345•I learned of a survey of 6049 (vaccinated and unvaccinated) women of whom many 292 (4.83% of respondents) reported a decidual cast shedding event, 277 of which had never been vaccinated (most of whom reported having been around vaccinated individuals).
Conversely, I have also come across cases of menstruation temporarily stopping, women becoming menopausal due to shedding.123456789 (or having permanently abnormal periods) and numerous cases where a shedding exposure may have ended a pregnancy (some of which were quite compelling).1234567891011121314151617
Note: while I am undecided on the miscarriage risk of shedding, based on the available data (and what I have directly observed), I am relatively sure COVID vaccination can cause miscarriages. Likewise, a few of my colleagues are now seeing vaccinated patients struggling to conceive (which greatly contrasts with what my colleagues had seen before the vaccines).
Other Bleeding
The second most common types of bleeding observed were:
•Nosebleeds1234. 56789101112131415161718192021222324252627282930313233 3435363738* 3940414243444546474849*5051525354555657•Painless and inexplicable bruising 1234. 56789101112131415161718192021222324252627282930313233 343536373839404142434445464748495051525354555657
Additionally, a few cases of gum bleeding1234, ear bleeding12 (including at the site of a previous piercing), eye bleeding (presumably from conjunctival hemorrhages)123456 were reported along with a reader who had bleeding hemorrhoids and one who had sporadic ovarian hemorrhaging.
Bleeding Mechanisms
I saw a few potential explanations to explain why this was happening.
First, as the above data (and many of the other observations of the vaccine) suggests, it could be hormonal, particularly since the vaccine’s lipid nanoparticles are known to accumulate in the ovaries (e.g., numerous readers reported ovarian pain after a shedding exposure1234).
While data is lacking in this area, a few women have reported measured hormonal levels changing after shedding exposures.123The best case report I know of comes from this reader, who regularly measured her hormones and repeatedly found her estrogen spiked after a shedding exposure. Conversely, another (50 year old) woman (who is also a physician) shared that after her shedding exposure, her estrogen and progesterone dropped to 0 (while some testosterone remained).
Note: numerous readers also reported breast cysts and tenderness from shedding.123
Second, it could be due to shedding directly causing bleeding, something supported by the non-menstrual types of bleeding, the fact that they often occurred in men (including one man who became anemic), that abnormal menstrual bleeding sometimes occurred concurrently with another type of bleeding (e.g., with nosebleeds), and that one women with post menopausal bleeding also had their prothrombin time increase.
While I suspect this was due to the spike protein damaging blood vessels, especially those near the surface of the body (e.g., in the nose), there were also cases suggesting it affected the blood cells themselves.
For example, someone with (well-managed) ITP (an autoimmune disease linked to vaccination that destroys your platelets) stayed at a vaccinated friend’s house. The next day, they had petechiae (lots of tiny spotted bruises) emerge and cover their entire face, so they went to the ER and learned their platelets dropped from normal levels (which range from 140,000-400,000) to under 2,000 and thus had to be in the hospital for 6 days to get their platelet levels back to normal levels (as they were at risk of a life threatening bleed)—something which also happened to another reader here (along with two other readers12 also experiencing ITP from shedding which I do not believe required hospitalization). Conversely, there was also a reader who had their platelet count instead become excessive (1.5 million). Lastly, there was also a case of hemolytic anemia.
Note: as far as I can tell, the male equivalents of female menstrual issues are (less frequent) testicular pain, groin pain,12 and nosebleeds.
Immediate Illness
After bleeding, the most common reaction individuals experienced was not feeling well after being in the vicinity of likely shedders.
Most commonly, this involved symptoms of a flu-like illness.1234567891011121314151617181920212223242526272829303132333435363738394041424344454647 48495051525354555657585960616263646566676869
Sometimes, those flu-like symptoms onset very rapidly, but in other cases people became ill the next day, and the illness could range from being brief, to lasting for months or becoming permanent. In numerous cases they reported being generally ill12 or “the sickest I’ve ever been.”
Sinus pressure or a copious nasal discharge was also frequently observed.1234.567891011121314151617181920212223242526272829303132333435363738
Swollen lymph nodes were also frequently observed.1234567891011121314151617181920
A variety of throat issues (e.g., pain in parts of the throat or difficulty swallowing12) were also reported.123456789101112Multiple readers also reported losing their voice for a prolonged period.1234
Many readers reported coughs that were typically chronic and dry, like those experienced in response to an irritant, or like those classically seen with an acute illness.1234567891011121314151617181920212223242526272829303132333435363738394041424344
Muscle pain, cramps or weakness were also often reported.12345678910111213141516171819* 20212223242526272829303132333435Night sweats were also sometimes reported.12345
In other cases, individuals developed COVID (in a manner strongly suggestive that it was due to shedding).123456789101112131415161718192021222324252627282930
Some of those COVID cases were quite severe123456, while others became long Covid,1234 and in some cases there were acute covid1 or long Covid relapses123 or vaccine injury relapses1 (something Pierre Kory has also observed within his patients).
Note: one bedside nurse shared that each time she had a COVID positive mother placed in isolation, she heard over and over, “My husband got the shot. He got sick and gave it to me.”
Inflammatory Symptoms
Many of the symptoms individuals reported overlapped with those reported from influenza or COVID. Still, they were more likely to be reflective of an inflammatory reaction or fluid congestion throughout the body (something that often follows these illnesses) rather than either disease.
The most common symptom reported were headaches.1234. 56789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127128129130131132133134135136137138139140
Typically, the headaches seemed to be similar to those experienced during the flu or inflammatory illnesses, but frequently were described as “migraines” and in some instances, “pressure,” sharp points of pain (suggesting blood stasis), or were associated with neck pain (suggesting tension headaches). This would be a classic example of a blood stasis headache:
Shortly after [my husband] received the vaccine, I started getting severe headaches, like nothing I had ever experienced before. It felt like a nail had been driven through my temple or eye, and my blood pressure would also spike at the same time. I have orthostatic hypotension and chronically low Bp, so this was notably unusual for me.
Additionally, body aches were sometimes reported along with one instance of shakes and dry heaves.
Fatigue was also frequently reported.12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364
This ranged from the fatigue and malaise felt during the flu, in a complete inability to do anything for days, to fibromyalgia triggering (or relapses of fibromyalgia and chronic fatigue123).
Two of the most common side effects of COVID vaccination were the spike protein causing an autoimmune disease and or it causing an exacerbation of a pre-existing one. This has also been seen with shedding, but not as frequently as after vaccination. For example:
Skin rashes are frequently reported after shedding exposures.1234. 5678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364656667686970717273
Most frequently these resemble hives, although a few people also reported psoriasis12 34, rosacea,1 shingles-like rash, and areas that felt like a rash but not was visible,1 2 or rosacea. Here are two examples of the rashes.12

Note: there was also one report of vitiligo—an autoimmune condition recently linked to vaccination in a large peer-reviewed study. Additionally, two reported becoming sensitized to sunlight,1,2something also seen in certain autoimmune conditions (e.g., lupus).
A variety of autoimmune diseases (e.g., rheumatoid arthritis) were reported to start or flare after shedding exposures).123456789Many also reported unspecified types of arthritis (which may have been immunologic in nature)1234567 or joint stiffness and one reported an exacerbation of ankylosing spondylitis.
Note: reoccurrence of pain at surgical site (another common COVID vaccine injury) was also reported.
Polymyalgia Rheumatica (a common COVID vaccine injury) was also repeatedly reported.12345
Many experienced severe (often stabbing) pain throughout the body,1234567 trigeminal neuralagia,1234 peripheral neuropathy123456789101112131415and signs of impaired sensation in the peripheral nerves (e.g., numbness or pins and needles).12345678910111213141516
Note: it’s hard to say if these nervous symptoms were due neural inflammation or inadequate blood supply to the nerves, as both can cause neuropathy and both follow COVID vaccination).
A variety of inflammatory nervous disorders were also reported such as Parsonage Turner syndrome (brachial neuritis), Transverse Myelitis, Ocular Neuritis and ADEM followed by behavioral changes, Multiple Sclerosis like symptoms123 (e.g., severe pain on the skin or sensitive skin) along with periodic electric pulses through the arms and legs (another MS symptom)—many of which I have also seen in vaccine injured patients.
Two individuals reported asthma exacerbations.12 Breathing issues1234567891011121314151617 and lung pain were also repeatedly reported. As chest pain or tightness was also reported123456789101112(along with numerous blood clots) it’s hard to say how many of these cases were due to an autoimmune response and how many were due clots in the lungs.
A few individuals reported anaphylactic responses,123 along with someone who would repeatedly have their veins collapse in the presence of shedders (and experience a vasovagal response).
One individual developed Sjögren’s syndrome while another had dry lips and mouth.
Two individuals developed lymphocitic colitis,12one developed type 1 diabetes (while two developed unspecified types of diabetes12) and one developed vasculitis. A variety of other organ injuries were also observed that could have been due to an autoimmune process or a lack of blood supply such as an acute kidney injury, kidney failure, IGA nephropathy, kidney pain and adrenal insufficiency, appendicitis and appendicitis symptoms, acute liver injury
Note a variety of individuals also developed gastrointestinal issues such as severe abdominal pain1,2,3 nausea (that is sometimes quite frequent), vomiting, bloating and moderate abdominal pain. 1234567891011121314151617181920212223242526272829303132333435
Lastly, hair loss has frequently been reported.123456789101112131415161718While it is unlikely this is due to hypothyroidism, acute thyroiditis, Hashimotos, goiter (thyroid enlargement), brittle nails and weight gain have also been reported.
Neurological Symptoms
A variety of neurological issues emerged, most of which were likely due to circulatory impairments and inflammation.
Tinnitus was one of the most frequently reported neurological symptoms.1234. 567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162636465Note: hearing loss was also reported.123
Dizziness was the other most frequently reported neurological symptom.1234. 5678910111213 1415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Note: loss of balance, hypotension, , lightheadedness, POTS123, and fainting1234 were also reported.
Brain fog and cognitive impairment, another common vaccine injury symptom was also repeatedly reported, although nowhere near as frequently as is seen in vaccine injured patients.1234567891011121314151617181920212223242526272829303132
•Eye issues were frequently reported such as partial vision loss345678910111213(frequently attributed to blood clots in the eyes), eye bleeds,123456 conjunctivitis, bloodshot eyes, dry eyes, burning eyes, double vision, blurry vision,12 eye lens turned opaque, numerous retinal detachments, vitreous detachment, floaters,12 and unspecified eye issues.1234
•Strokes,12345 (including in a child), clinical signs of a stroke (without a diagnosis), arm weakness, and Bell’s palsy.123456
Note: Justin Bieber (who also had chronic Lyme disease) and then a severe form of shingles in association with COVID vaccination was the most well-known incidence of COVID vaccination preceding Bell’s palsy.
•Seizures,12345 including one that was fatal.
Internal Vibrations123, (an unusual symptom which has been linked to long COVID and vaccine injuries), a shaking, buzzing, or feeling as though fireworks were going off inside the body,12345 one case of exploding head syndrome (a non-dangerous disorder where individuals inexplicably hear very loud noises like a firecracker going off as they fall asleep), and brain zaps (something commonly associated with SSRIs).
Finally, one reader also reported a suspected link between misophonia (extreme emotional responses to certain sounds) and shedding.
Circulatory Symptoms
In addition to the neurological symptoms, other circulatory issues were also reported:
•The heart issues were primarily chest pain, angina and tightness,123456789101112131415 atrial fibrillation,123456789101112 along with heart palpitations, arrhythmias, tachycardia or PVCs.1234. 567891011121314151617181920212223242526272829303132333435363738394041424344454647
•A few heart attacks,12345myocarditis12345 (including a fatal case and myocarditis following blood transfusion), pericarditis,12 pericardial effusion, cardiomegaly, possible heart failure, pre-existing cardiomyopathy worsening.
•Severe blood clots,123456789101112 some of which were life threatening (e.g., pulmonary embolisms) and resembled those seen after the vaccine. Additionally, clots were reported in one cat and many minor clots have been observed as well.123
•Raynaud’s,12345peripheral arterial disease, lumps on blood vessels, and an acupuncturist reporting that her limbs, abdomen and veins will consistently turn blue 4-6 hours after working with triple-vaccinated patients.
•A hypertensive emergency and elevated blood pressure.
Note: May-Thurner syndrome (for 2 months) and symptoms suggestive of erythromelalgia or venous insufficiency (e.g., feeling like one’s blood was on fire, severe insomnia, extreme cold and cold aversion, sun sensitivity, swollen red and dry looking veins) were also reported.
Immune Suppression
Additionally, a subset of readers appeared to develop immune suppression due to shedding.
As shingles is one of the most common illnesses triggered by immune suppression, it has also been the most common one triggered by vaccination and shedding.1234.5678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455
Activations of herpes,1234567Lyme disease,1234567Epstein Barr123456789 have also been repeatedly reported.
Note: reactivations of Epstein Barr and herpes have been repeatedly observed in COVID vaccine injured patients.
Many patients have reported a chronic susceptibility to illness after vaccination12345678910 (including in a child and one case where serial lab work showed shedding repeatedly caused immune suppression).
Lethal pneumonia, near lethal pneumonia through secondary shedding, bronchopneumonia, and unusual bacterial infections.
Note: lastly, an oral mucocele (blood blister), cherry angiomas, styes and eyelid swelling,12 tendon and ligament issues,12 a pelvic prolapse and a tooth lost to resorption have also been reported.
Menstrual Shedding Data
In addition to the reports compiled through social media, MyCycleStory conducted an IRB approved study of 6049 female respondents (18 and older) which identified 3390 who had never had COVID-19 or a vaccine, and found 92.3% of them experienced menstrual abnormalities likely due to shedding which typically onset within 3 days of exposure:
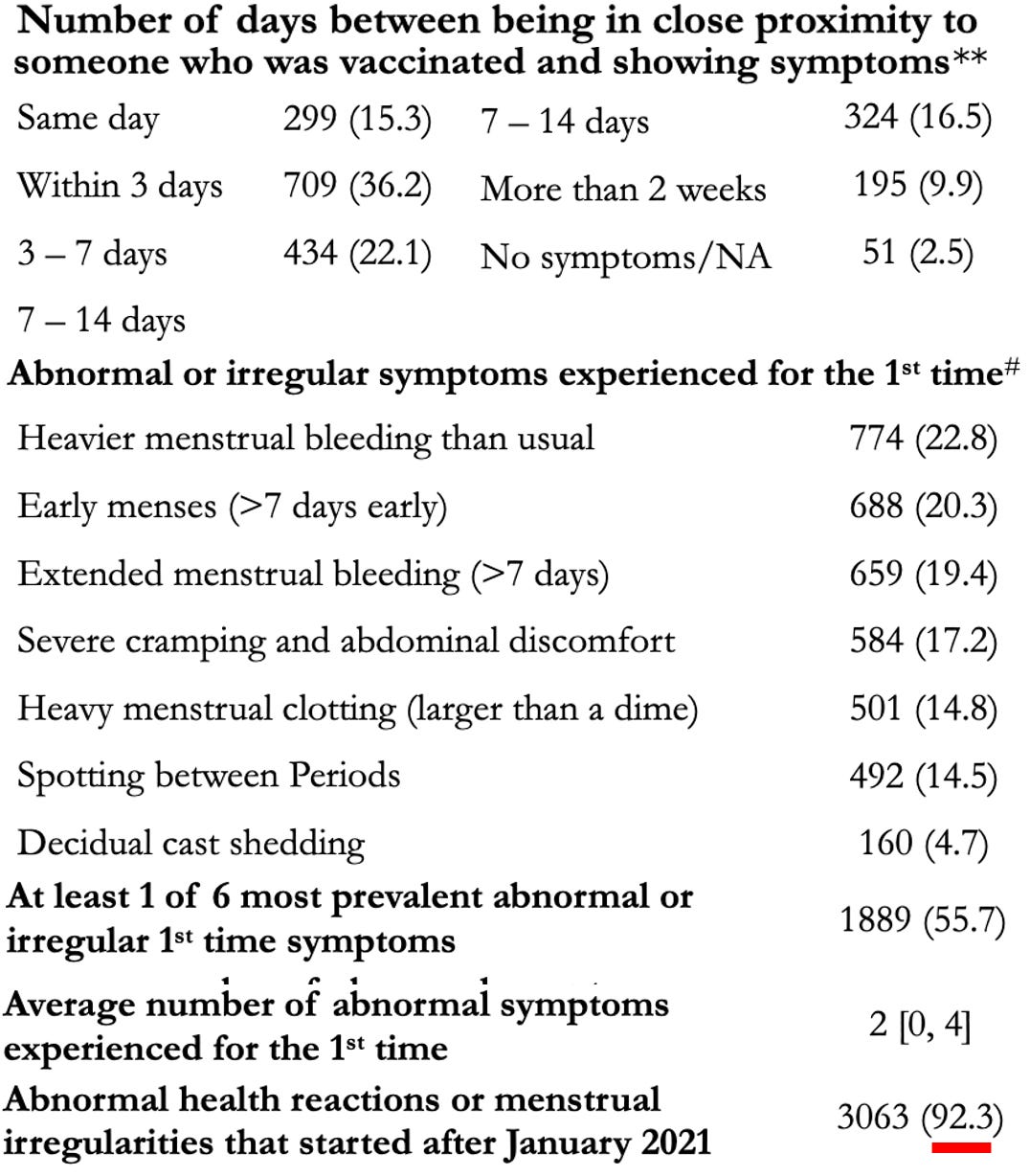
Additionally, they found these symptoms were strongly associated with shedding exposures:
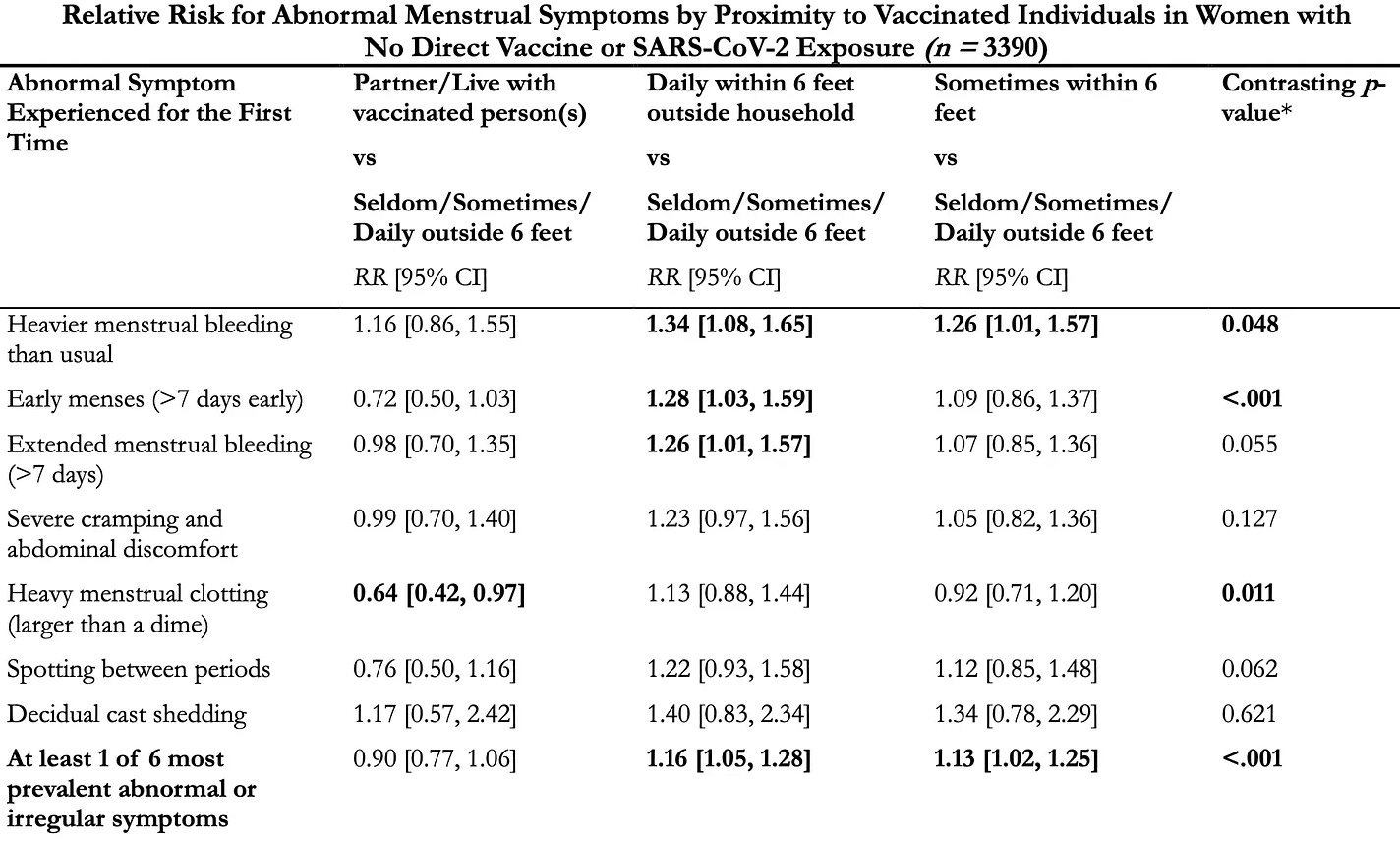
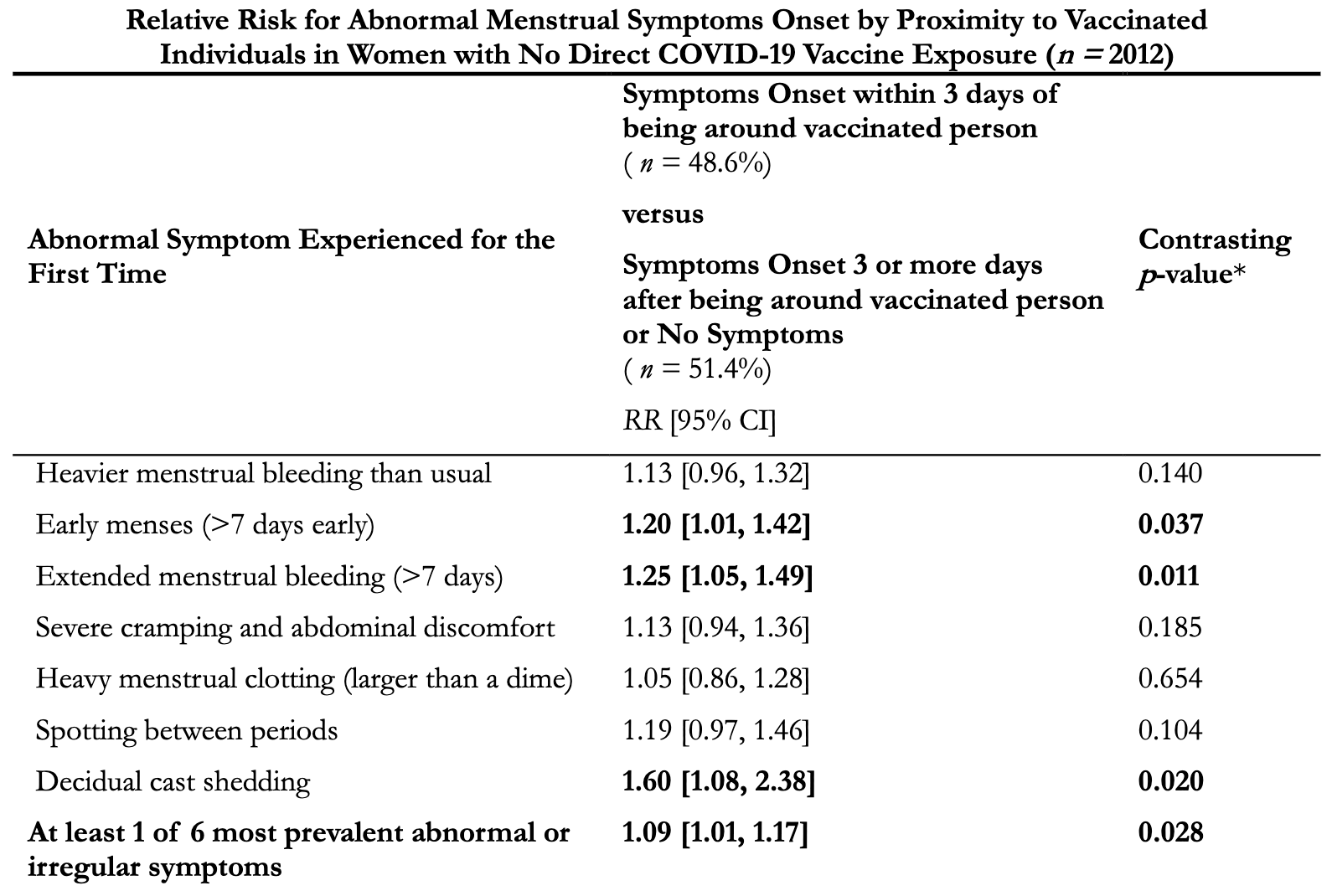
Given how strong the associations are here (as almost everyone had these symptoms start after the COVID-19 vaccine roll-out) and how hard it is to conduct studies like this in the current political climate, I believe the case has been made (until data shows otherwise) that:
•The other common shedding symptoms detailed in this article would also show a similar strong association with being exposed to vaccinated individuals.
•Were a more sensitive study to be conducted, that many of the less frequent symptoms would be as well.
POLL
Based on the information in this article, do you believe you have been affected by COVID vaccine shedding?
Yes
Yes, and I was significantly harmed
Possibly
No
I have no idea
365 VOTES ·
The Mechanistic Trap
A major problem with modern science is that things (including those you see with your own eyes) are assumed to not exist unless an agreed upon mechanism exists to explain them. As such, I frequently will observe things (e.g., shedding) I can tell exist, but will be vociferously denounced by my peers for endorsing—despite the fact existing mechanisms are routinely disproved (e.g., depression is not a chemical imbalance) and new ones are regularly discovered.
Note: the mechanistic trap is often utilized to string together a series of misleading premises to assert a scientific orthodoxy (e.g., that the COVID vaccines “do not persist in the body” or that “they cannot change your DNA”) rather than providing data to establish the assertion.
As such, a key focus has been on identifying mechanisms that could explain shedding.
Is Shedding Possible?
Typically, shedding occurs (e.g., from a live viral vaccine like MMR or polio) because an individual “sheds” a self-replicating form of the disease. This results in a low concentration of the pathogen, which the shedder expels into their environment, then amplifies within the recipient and eventually reaches a comparable concentration to what was found in the “shedder.”
However, the mRNA vaccines do not contain self replicating pathogens, so limited options exist for what could spread, none of which make sense. For example:
•It’s possible some of the vaccine nanoparticles are excreted (especially when someone was recently vaccinated), but so few exist to begin with that it is unlikely that enough could ever be excreted to affect someone (let alone for an indefinite period), particularly since they cannot penetrate the skin, but many have reported reacting to touching surfaces shedders have contacted.
•If the spike protein produced by the vaccine is being shed, it seems nearly impossible that one’s tolerance to it could vary so greatly that one person could be asymptomatic from a large number of spike protein inside them, but another could become ill from the small amount that periodically exit that person and then are massively diluted in the environment.
At the same time however, Pfizer’s protocol for testing their vaccine:
- Prohibited pregnant women or those breast feeding from receiving the vaccine (or future doses if they had already received one).
- Stated it needed to be reported if a pregnant women (e.g., a healthcare worker in the trials) was exposed to the intervention by inhalation or skin contact from someone who had been vaccinated.
- Stated it needed to be reported if someone in the previous category (not vaccinated but exposed to someone who was) then was in close proximity to their wife and their wife was pregnant.
This suggested either that Pfizer knew shedding (and secondary shedding) was a real problem, or that they were following the existing standards—the FDA stipulates that gene therapies need to be evaluated for shedding before being given to humans (and furthermore be subsequently tested for shedding in humans). For context, both the FDA and the EMA (along with Moderna and Pfizer 1,2,3) classify the mRNA vaccines as a gene therapy.
Note: the first approved gene therapy, Luxturna, (which works like the J&J vaccine by using a modified virus to produce a target protein in the patient), is an eye medication (that costs $425,000.00 per eye) that treats a rare form of genetic vision loss (that DMSO also treats). Its prescribing information specifies that Luxturna can be found in a patient’s tears after injection. Hence, for the first seven days after injection, care must be taken to prevent anyone else from coming in contact with those tears and to prevent unintended shedding of the product. Another similar gene therapy, Roctavian was also found to shed (e.g., into semen), and the FDA advises those who receive it not to donate semen or impregnate someone for at least 6 months after administration. Finally, Zolgensma, a gene therapy, utilizing a different virus was also found to shed for a month, and its package insert advises that during this time, to be careful of how feces from the patients are disposed of (so no one else is exposed to it). Additionally, there is one other gene therapy on the market, but due to its design, shedding was unlikely (and hence undetected) so the FDA does not advise special precautions for its recipients. Curiously, the package inserts for all of the American COVID vaccines do not mention shedding.
Shedding Mechanisms
Note: a previous article provides important additional context for this section.
At this point, I have identified three viable shedding mechanisms which can account for the existing data.
Exosome Mediated Shedding
Exosomes are small spheres continually released from cell membranes to communicate with their surroundings (many vital processes are regulated by exosomes) and transport intercellular contents. Mothers for example have exosomes in their breastmilk which make it through the digestive tract and deliver [micro]RNA to their developing babies which plays a critical epigenetic role in guiding their healthy development).
Note: exosomes are very similar to and inspired the creation of lipid nanoparticles (which were used to make the COVID vaccines).
One of the unique aspects of COVID-19 is that it “poisons” the exosome system.1,2,3,4,5
In turn, at the start of the pandemic, it was discovered that using therapeutic (healthy) exosomes produced dramatic results from severe COVID-191,2,3 and numerous people I am close to almost certainly would have died had we not given them therapeutic exosomes.
Later, it was discovered that the COVID vaccine also poisons the exosome system, which I believe is primarily due to the mRNA vaccine overproducing spike proteins which then get pushed out of the cells onto their membrane (at which point they bud off into spike protein studded exosomes). Additionally, those exosomes may also contain either vaccine mRNA or plasmids.

Note: the negative controls in the above experiment did have spike protein on their exosomes.
Presently, it has been shown that:
•Spike protein containing exosomes (which circulate in the bloodstream) spike after vaccination (and then decline) and appear to be one of the primary things responsible for triggering the immune response that creates antibodies to the vaccine, as once spike protein coated exosomes are transferred to mice, the mice develop antibodies to the spike protein (along with increasing levels of various inflammatory cytokines).
•A 2023 peer-reviewed study found that unvaccinated children who were around COVID-19 vaccinated parents developed an immune response to the spike protein that was not seen in children with unvaccinated parents—which meant something was indeed being shed. Additionally, they were also able to find spike protein antibodies in surgical masks worn by the physicians. This led the authors to hypothesize that antibodies were being directly transferred through the parent’s breath to their children.
•Significant amounts of (RNA containing) exosomes can be found in your breath, and those exosomes (which derive from the lungs) vary depending upon on the disease state someone has (“sicker” people have “worse” exosomes).1,2,3
Note: since this is a relatively new field of research, each paper is more sophisticated than the preceding one.
•As I showed in this article, there was significant variation in how the COVID vaccines were produced (e.g., that’s why there were “hot lots”), which caused some batches to concentrate in the lungs. In theory, this means that a portion of vaccine recipients could have briefly exhaled much of their vaccine (including the spike protein producing mRNA).
•The spike protein has a high (heparin dependent) affinity for binding to the surface of exosomes. So, if it was not already there when the exosome initially formed, it can also attach to exosomes traveling in the bloodstream.
•Long COVID (and more severe acute COVID) is characterized by the presence of spike protein studded exosomes (see this paper and this paper). Additionally, they also showed exosomes from COVID patients are highly inflammatory (and potentially clot forming) and are taken up by the lung cells. The most detailed study (and imaging) of spike protein containing exosomes can be found in this paper (which also found that spike protein containing exosomes can circulate a year after COVID infection).
Note: this study also found that COVID triggers the production of spike protein-coated exosomes, and when lung cells are exposed to those exosomes, an immune response to the spike protein is triggered.
•An inhaled vaccine was made from lung derived exosomes coated with spike proteins (they were lung derived so the lung cells would be more likely to absorb them). These spike protein exosomes both generated an immune response and were absorbed into the body. Once absorbed, those exosomes travel to other tissues and organs in the body, which (based on all the reports we’ve received and the patients we’ve seen) are known to be affected by shedding.
Collectively, this suggests that vaccinated individuals are continually exhaling spike protein studded exosomes, and that those around them are either inhaling them or touching surfaces they contacted, and then reacting either to the pathologic spike proteins on the exosomes (more likely), or taking up the exosome content and effectively being vaccinated with vaccine mRNA the exosomes traffic into their cells (less likely).
I find this theory compelling as it matches most of the available data, addresses the concentration issue (as what’s exhaled is comparable to what’s inhaled), and explains how a shedder can continuously produce the shedding agent (provided the vaccine mRNA persists). The major issue with it is that both exosomes and the spike protein have limited penetration through the skin (while no data exists on both together), so it is unclear if the allergic response alone that the spike protein generates could be sufficient to create the immediate reactions many have had to touching shedders.
SARS-CoV-2 Shedding
In a significant number of the reports I looked at, after being exposed to an (asymptomatic) shedder, the individual (and often multiple other unvaccinated members of the group) became ill with one or more of the following:
•COVID-19
•A COVID-like illness
•A flu which may have been COVID
•A severe COVID infection that hospitalized and sometimes killed them.
Yet in contrast, before the vaccine rollout, they never had this issue (e.g., normally they never got sick, even around those they knew got COVID). This in turn, means either that a remarkable coincidence keeps on happening, or that the vaccine increases your risk of transmitting COVID-19.
As it so happens, there are a few things that argue for the latter such as:
•The design of the vaccine does not create mucosal IgA immunity. This means it does not prevent COVID-19 from colonizing the respiratory tract and hence makes one still able to spread COVID-19.
•The vaccine’s design primarily reduces reactivity to the spike protein (i.e., COVID-19 symptoms). As such, vaccinated individuals can be infected with COVID-19 but not show symptoms of infection.
•The vaccine is immune suppressing. On one hand, this results in individuals who have a latent COVID infection becoming severely ill (which as I show here is a common but forgotten problem with vaccines). On the other hand, it causes individuals who have been vaccinated to be unable to develop permanent immunity and, hence, continually catch it.
Note: I have received many reports of vaccination causing an existing minor COVID infection to become life threatening,
In short, for some reason, individuals who do not get COVID will come down with it in the presence of a shedder, and in my assessment, this happens frequently enough for it not to be a simple coincidence.
Based on all of this, it seems plausible that vaccinated individuals with COVID infections either excrete higher concentrations of the spike protein than those with natural immunity, or have chronic infections they never clear (but show minimal symptoms of). However, the existing data on the length of infectiousness and viral counts in the noses of those infected with COVID-19 (which may be biased) shows minimal differences between the vaccinated and unvaccinated. As such, while it seems that vaccination causes certain individuals to give others COVID, to the best of my knowledge data does not exist to support that claim and there may be some other process concurrently occurring which makes those around a shedder more susceptible to catching COVID-19 from them.
Plasmid Contamination
The third potential shedding vector are its DNA contaminants. Briefly, to mass produce the vaccine, a process (that was never tested for safety) was utilized to create synthetic bacterial DNA (plasmids), mass produced bacteria with those plasmids, and then used those plasmids to synthesize the vaccine mRNA. The problem with this approach was that the synthetic DNA was not fully removed from the vaccines, so many were injected not only with mRNA but also foreign DNA (which was uniquely suited to enter the nucleus and potentially integrate with the human genome due to its having the SV-40 promoter).
These plasmids in turn, made it possible for something to be “shed” from the vaccines that could then infect the recipient and reproduce in them (thereby making the minuscule amount shed have clinical consequences). This in turn, could either happen by:
1. Exhaled exosomes containing the plasmids, which then found they way into the cells after they were inhaled and then were able to enter the nucleus of cells and cause them to become spike protein factories (which I feel is fairly unlikely).
2. The plasmids transfecting the microbiome of the vaccine recipient, those bacteria reproducing the plasmid (which can then transfect other bacteria), and then those bacteria being shed to others (either causing them to produce the spike protein or to simply be dysfunctional). This theory is compelling as it:
•Allows for self-replicating pathogen to be “shed” (hence fulfilling the classic requirement for a vaccine to be able to “shed”).
•Can easily allow transmission to occur both by touch (as bacteria are on the skin), by simply being in the presence of the shedder (as humans are surrounded by a cloud of their microbiome).
•Makes secondary shedding possible as the transfected bacteria could linger on someone who’d been shedded on, in the air shedders had breathed, or the surfaces they’d touched (e.g., sheets).
The major problem with this theory is that to the best of my knowledge, there is no published data to support or refute it (as doing so would be expensive and require specialized technology). Rather, the closest things I know of were:
•A study of 34 individuals which found that before vaccination, bifidobacteria composed1.13% of their gut microbiome, whereas 1 month after vaccination, it was 0.64% of their microbiome (a 43.36% decrease).
•A study of 4 individuals found that this decrease increased with time, dropping by 73% at 6-9 months out.

These results are both important due to the importance of bifidobacteria for general health and susceptibility to COVID-19 (as this highlights another danger of COVID vaccination) and because it shows that the vaccine can create long-term alterations in the gut microbiome—which could potentially be attributed to plasmid alternations of it.
Note: it is now known that the most dangerous vaccine lots also had higher amounts of the plasmid contaminants.
Other Mechanisms
Of the three previously listed mechanisms, based on all the available information (including what could account for the 1,500 reports I read through) I believe exosome mediated shedding is the most probably culprit, while spike protein expressing bacteria best addresses the unanswered questions about shedding (but still lacks the evidence to corroborate it).
Additionally, I have also come across three other potential mechanisms (which for a variety of reasons I believe to be less likely):
•Exhalation of toxic lipid nanoparticle breakdown products (e.g., PEG).
•Pheromone mediated “shedding” (as women’s menstrual cycles can be quite sensitive to the pheromones of those around them).
•An energetic quality (likely mitogenic radiation—which I discussed in detail here) is emitted by shedders directly affecting the physiology and cellular activity of those around them.
The Cost of Shedding
This has been one of the more challenging articles here to write, in part because of how much data needed to be synthesized but also because many of these stories (especially the cancer ones) are quite heart wrenching and challenging to bear witness to.
Furthermore, given how inexplicable many of these symptoms appear, the selectivity in which they affect only certain people and the belief mRNA shedding is “mechanistically impossible” it naturally leads to those suffering from it to be relentlessly gaslighted. For a moment, consider what some of these people are going through:
My wife also experienced some reproductive difficulties as well. Neither one of us is vaccinated. The doctor told her it was in her head, so we both stopped talking about it.
[I experienced] shedding from a massage therapist who, while I was on the table, told me I was “safe” because she just had her booster. I got terribly sick.
It happened to me. This is why I haven’t gone out since 2021, even after I had covid in 2022 I still stay home. Nothing non-essential is worth disrupting my menstrual cycle again.
I never got sick throughout the Covid madness. Now every time I’m around the vaxxed in social gatherings I get sick.
My unvaxed friend had to stop going to church because the entire congregation was vaxed and she got sick every time she went.
Note: in 2021, a Miami school generated significant controversy by prohibiting students from attending the school within 30 days of vaccination.
At the same time, we also must consider an even more uncomfortable question. Has shedding inflicted large scale harm on the population? Given the controversial nature of this topic, it is understandable that it would rarely if ever be studied. However:
•One research paper (which, given its content has been indefinitely stuck in pre-print limbo) discovered in multiple countries that when adults received the COVID vaccine but no one under 18 was being vaccinated, death rates significantly increased in children.
•That same pattern was also detected by another researcher in the Phillipines.
•To evaluate the effects of shedding on the unvaccinated, one researcher analyzed England’s data (as it is one of the most comprehensive available datasources). In it, she found that during vaccine campaigns, the ratio between non-COVID to COVID deaths significantly increased (suggesting the vaccine was causing people to die) and that this increase was also seen in the unvaccinated—to the point it was arguable shedding killed more unvaccinated than COVID-19 did.
In short, while it is grossly unethical to mislead or force individuals into taking an unsafe and ineffective pharmaceutical, it is even more unethical to harm those who did not consent to it in the first place (e.g., this is why I’ve felt compelled to speak out about SSRI antidepressants causing psychotic violence and mass shootings).
As such, my hope is that I have made the case that mRNA technology must be subject to the same shedding evaluation requirements other gene therapies are, and that robust data on any potential shedding risks must be made publicly available before any new mRNA injection can come to market.
Furthermore, reestablishing the importance of this is now more critical than ever as the widespread opposition to vaccination we are now seeing has paralleled an increasing disregard for ethical principles by the medical profession (e.g., numerous recent publications have argued for the “ethics” of vaccine mandates). In turn, since mandates are becoming politically unviable, the medical field is looking into other ways to “bypass” vaccine hesitancy, such as self-spreading vaccines, which rapidly disseminate throughout the population (including those who did not want to vaccinate).
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Moving Forward
While all of this is highly depressing, in my eyes, there are three major bright sides to it.
First, I am almost certain that in any previous era, COVID-19 vaccine shedding would have been dismissed as a fringe conspiracy theory and entirely forgotten by anyone not permanently affected by it. Due to the new era of media we are in and platforms like Substack making it possible to collate and share large volumes of information, many people now recognize that shedding is real, and articles like this can gain significant traction. I cannot understate how profound of a shift this is as nothing like that has ever been possible. Likewise, it will be much more difficult for the pharmaceutical industry to enact its predatory tactics in the future.
Note: due to the blitzkrieg used to sell the COVID vaccines, a few years ago, being COVID vaccine injured was taboo and not unlike being a gay person in the closet in the 1980s —whereas in just a few years it remarkably has become an open topic of discussion. At that time, it was impossible to publish anything about vaccine injuries, so I decided to compile an extensive log of injuries within my personal circle and later anonymously publish it so the injured could see they were not alone and help start the ball rolling towards acknowledging vaccine injuries. A year ago, I felt shedding injuries were in the same place COVID vaccine injuries were a few years prior (hence why I took this project on), and while it has not come as far as vaccine injuries, a year later it is no longer a taboo topic to discuss—which is a truly remarkable speed of social change.
Second, the effects of shedding generally decrease the further one is from vaccination. Since the COVID vaccine program is dying, this will be less of an issue as time progresses.
Third, shedding provides one of the strongest arguments against future mRNA vaccination campaigns (which is why it must be exposed). All other gene therapies are given in limited contexts, and maximum precautions are taken to ensure they are not shed on unintended recipients. We must do everything possible to ensure this same standard applies to mRNA vaccines. As such, if you are a researcher, I would greatly appreciate if you could review the data shared here and share your own analyses (I’ve put hundreds of hours into this, and I’m at the limit of what I can do), while if you have experienced shedding (and not yet shared your story) to do so.
In the final part of this article I will go into a few lingering questions we are still a bit hesitant to publicly approach, such as how shedding affects sexual intimacy, cancer (some of the stories are quite sad), the safety of blood transfusions, and the methods we have found to mitigate the impacts of shedding.